

Introduction:
The standard approach for relapsed or refractory (RR) classical Hodgkin lymphoma (cHL) following front-line treatment failure is second line therapy (SLT) aimed to achieve complete response (CR), followed by consolidation with high dose therapy and autologous hematopoietic cell transplantation (HDT/AHCT). No one standard SLT exists and options include regimens containing platinum, gemcitabine, and more recently brentuximab vedotin (BV). Complete response rates associated with these regimens range from 50-70%. Due to the increasing use of BV in the front-line setting, development of SLT regimens that are both highly effective and BV-sparing are needed. Programmed death-1 (PD-1) inhibitors are highly active in RR cHL and have the potential to enhance the efficacy of standard chemotherapy. Here we report the results of our phase II study evaluating a novel anti-PD-1-based regimen, pembrolizumab plus gemcitabine, vinorelbine, and liposomal doxorubicin (pembrolizumab-GVD), as SLT for RR cHL.
Methods:
Transplant eligible patients (pts) with RR cHL following failure of 1-line of therapy were eligible. Treatment consisted of 2 to 4 cycles of pembrolizumab (200mg IV, day 1), gemcitabine (1000mg/m2 IV, days 1 and 8), vinorelbine (20mg/m2 IV, days 1 and 8) and liposomal doxorubicin (15mg/m2, days 1 and 8), given on 21-day cycles. Pts who achieved CR by PET (Deauville ≤3) after 2 or 4 cycles proceeded to HDT/AHCT. HDT/AHCT was carried out according to institutional standards and BV maintenance was allowed following HDT/AHCT. The primary endpoint was CR rate after 2 or 4 cycles of pembrolizumab-GVD. Enrollment occurred according to a Simon 2-stage design with sample size based upon a projected CR rate of 70%. In stage 1, 23 pts enrolled and 12 or more CRs were required to proceed to stage II; in stage II, an additional 16 pts enrolled. Out of a total of 39 pts, 24 CRs were required to declare this regimen promising.
Results:
Among 39 patients enrolled, 37 are evaluable for toxicity (2 pts have not yet started treatment) and 34 are evaluable for response (4 pts too early, 1 pt found to have composite lymphoma after enrollment). Of 37 treated pts, median age is 36 (range 21-71), 43% are male, 23 (62%) had advanced stage disease, and 15 (41%) had primary refractory disease. With regard to RR cHL risk factors (B-symptoms, extranodal disease, and relapse/refractory disease within 1 year of initial treatment), 4(11%) had no risk factors (RFs), 21 (57%) had 1 RF, 9 (24%) had 2 RFs, and 3 (8%) had all 3 RFs.
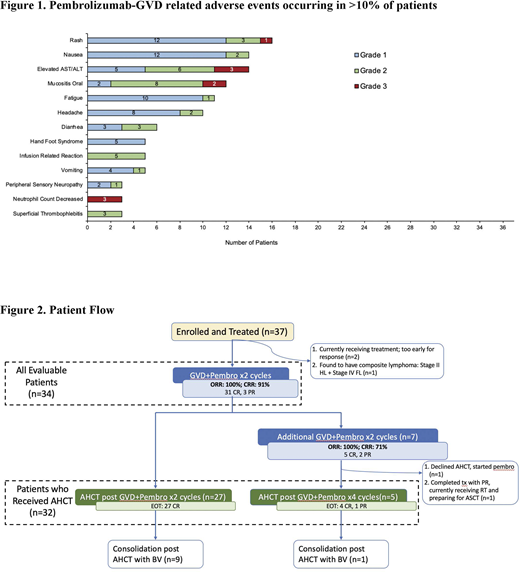
Treatment was well tolerated with most adverse events being grade 1 or 2 (see figure 1). Grade 3 AEs included rash (n=1), elevated AST/ALT (n=3), oral mucositis (n=2), and neutropenia (n=3).
Figure 2 shows the outcome for all 37 treated pts. Among 34 evaluable pts, 31 (91%) achieved CR after 2 cycles and 3 achieved partial response. An additional 1 pt achieved CR after 4 cycles of pembrolizumab-GVD, therefore in total, 32 of 34 (94%) achieved CR following pembrolizumab-GVD. 4 pts with CR after 2 cycles received an additional 2 cycles of pembrolizumab-GVD in order to delay HDT/AHCT during the height of the COVID-19 pandemic (n=3) or due to refusing HDT/ASCT (n=1). To date, 32 have undergone HDT/AHCT following 2 (n=27) or 4 (n=5) cycles of treatment. 1 pt is awaiting HDT/AHCT; 1 pt refused HDT/ASCT and received pembrolizumab maintenance instead. 2 pts received involved site radiation therapy to initial area of relapsed disease prior to planned HDT/AHCT and 10 pts received post-HDT/ASCT maintenance with BV. Median follow-up post-HDT/AHCT is 9 mos (range 0.03-20.9 mos) and all pts remain in remission to date.
Conclusion:
Second-line therapy with pembrolizumab-GVD is a highly effective and well-tolerated regimen that can efficiently bridge pts with RR cHL to HDT/AHCT. Updated results including all 39 enrolled pts will be presented at the meeting. Given the high CR rate observed with pembrolizumab-GVD, an expansion cohort evaluating 8 cycles of pembrolizumab maintenance (instead of HDT/AHCT) for patients who achieve CR after 4 cycles of pembrolizumab-GVD is planned.
Moskowitz:Merck: Consultancy; Incyte: Research Funding; Miragen Therapeutics: Consultancy; Seattle Genetics: Consultancy; Imbrium Therapeutics, L.P.: Consultancy; Merck: Research Funding; Seattle Genetics: Research Funding; Bristol-Myers Squibb: Research Funding. Shah:Amgen Inc.: Research Funding; Janssen: Research Funding. Kumar:AbbVie: Research Funding; Celgene: Honoraria, Other: Honoraria for Advisory Board; Seattle Genetics: Research Funding; Astra Zeneca: Honoraria, Other: Honoraria for Advisory Board; Celgene: Research Funding; Kite Pharmaceuticals: Honoraria, Other: Honoraria for Advisory Board; Adaptive Biotechnologies,: Research Funding; Pharmacyclics: Research Funding. Lahoud:MorphoSys: Other: Advisory Board. Batlevi:Life Sci, GLG, Juno/Celgene, Seattle Genetics, Kite: Consultancy; Janssen, Novartis, Epizyme, Xynomics, Bayer, Autolus, Roche/Genentech: Research Funding. Hamlin:J&J Pharmaceuticals: Research Funding; Portola: Research Funding; Incyte: Research Funding; Portola Pharmaceutics: Consultancy; Juno Therapeutics: Consultancy; Karyopharm: Consultancy; Celgene: Consultancy; Molecular Templates: Research Funding. Straus:Karyopharm Therapeutics: Membership on an entity's Board of Directors or advisory committees; Imedex, Inc.: Speakers Bureau; Targeted Oncology: Consultancy, Speakers Bureau; NY Lymphoma Rounds: Consultancy; Takeda Pharmaceuticals: Research Funding, Speakers Bureau; OncLive: Speakers Bureau; Elsevier: Membership on an entity's Board of Directors or advisory committees, Other: CME writer; ASH: Other: Conference in December 2019 on HL to other physicians during ASH; Seattle Genetics: Consultancy, Membership on an entity's Board of Directors or advisory committees. Horwitz:ASTEX: Consultancy; Verastem: Consultancy, Research Funding; Myeloid Therapeutics: Consultancy; Miragen: Consultancy; Kura Oncology: Consultancy; Janssen: Consultancy; GlaxoSmithKline: Consultancy; Daiichi Sankyo: Research Funding; C4 Therapeutics: Consultancy; Affirmed: Consultancy; Vividion Therapeutics: Consultancy; Beigene: Consultancy; Portola: Consultancy, Research Funding; Mundipharma: Consultancy; Innate Pharma: Consultancy; Corvus: Consultancy; Trillium: Consultancy, Research Funding; Seattle Genetics: Consultancy, Research Funding; Millenium/Takeda: Consultancy, Research Funding; Kyowa Hakka Kirin: Consultancy, Research Funding; Infinity/Verastem: Research Funding; Forty Seven: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Aileron: Consultancy, Research Funding; ADCT Therapeutics: Consultancy, Research Funding. Falchi:Genmab: Research Funding; Roche: Research Funding. Joffe:Epizyme: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Membership on an entity's Board of Directors or advisory committees. Noy:Pharmacyclics: Research Funding; Pharmacyclics: Consultancy; Janssen: Consultancy; Rafael Pharma: Research Funding; NIH: Research Funding; Morphosys: Consultancy; Medscape: Consultancy; Targeted Oncology: Consultancy. Matasar:Teva: Consultancy; Genentech, Inc.: Consultancy, Honoraria, Research Funding; Merck: Consultancy; Bayer: Consultancy, Honoraria, Research Funding; Juno Therapeutics: Consultancy; F. Hoffmann-La Roche Ltd: Consultancy, Honoraria, Research Funding; GlaxoSmithKline: Honoraria, Research Funding; IGM Biosciences: Research Funding; Janssen: Honoraria, Research Funding; Pharmacyclics: Honoraria, Research Funding; Immunovaccine Technologies: Honoraria, Research Funding; Rocket Medical: Consultancy, Research Funding; Takeda: Consultancy, Honoraria; Daiichi Sankyo: Consultancy; Seattle Genetics: Consultancy, Honoraria, Research Funding. Vardhana:Other: Other: SAV has received honoraria from Agios Pharmaceuticals and Rheos Pharmaceuticals, is an advisor for Immunai and has consulted for ADC Therapeutics. von Keudell:Genentech: Research Funding; Bayer: Research Funding; Pharmacyclics: Research Funding. Zelenetz:Novartis: Consultancy; Janssen: Consultancy; Celgene: Consultancy; Amgen: Consultancy; Adaptive Biotechnology: Consultancy; BeiGene: Membership on an entity's Board of Directors or advisory committees; Roche: Research Funding; Gilead: Research Funding; Genentech/Roche: Consultancy; Gilead: Consultancy; Sandoz: Research Funding; Celgene: Research Funding; MEI Pharma: Research Funding; MorphoSys: Research Funding.
Pembrolizumab as second-line therapy for Hodgkin lymphoma

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal